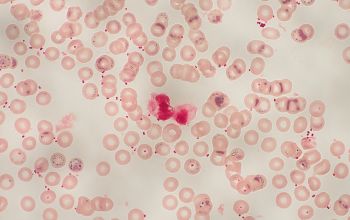




Waterhouse-Friderichsen syndrome
photo Prof Hubert P. Endtz

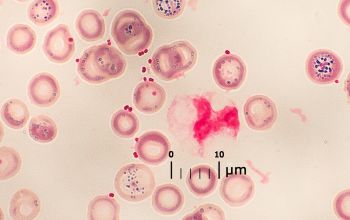
Waterhouse-Friderichsen syndrome
photo Prof Hubert P. Endtz

Neisseria meningitidis
-
General information
Taxonomy
Family: Neisseriaceae
Natural habitats
N. meningitidis occurs exclusively in humans and plays a dual role of commensal and potential invasive pathogen.
On average, the mucosal surfaces of oro- and nasopharynx of 10% of the population is colonized by this bacterium.
Carriage is strongly age dependent, with adolescents and young adults attaining rates of over 30% in contrast to infants with carriage rates of a few percent.
Transmission occurs through droplet secretions from the oropharynx and close contact.
Clinical significance
They can cause meningitis and other forms of meningococcal disease.
Meningitis symptoms
Fatigue, fever, and headache and can rapidly progress to neck stiffness, coma and death in 10% of the cases.
Meningococcal septicemia
Typically causes a purpuric rash, that does not lose its color when pressed with a glass (“non-blanching”) and does not cause the classical symptoms of meningitis.
This means the condition may be ignored by those not aware of the significance of the rash. Septicemia carries an approximate 50% mortality rate over a few hours from initial onset.
Waterhouse-Friderichsen syndrome
Is adrenal gland failure due to bleeding into the adrenal glands, caused by severe bacterial infection, most commonly, N. meningitidis
-
Diseases
-
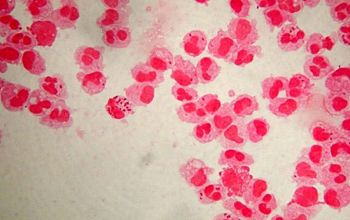
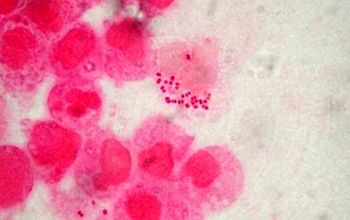
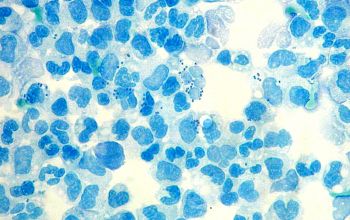
Gram stain
Gram negative diplococci,
"Kidney bean" or "coffee bean" shaped cocci
Occuring singly or in pairs with adjacent sides flattend.
They appear both inside and outside polymorph nuclear leukocytes and may tend to resist decolorization.
Capsule may be present
-
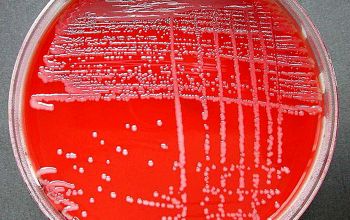
Culture characteristics
-
Obligate aerobic
5% CO2 improves the growth
BA: after 18 hours, colonies are 1mm, smooth, gray, convex, glistening and occasionally mucoid.
Blood agar beneath the colonies may display a gray-green color.
McConkey: no growth
BBAØ: no growth
-
-
Characteristics
-
References
James Versalovic et al.(2011) Manual of Clinical Microbiology 10th Edition
Karen C. Carrol et al (2019) Manual of Clinical Microbiology, 12th Edition
Microbiology on the go. An initiative by
Dept. Medical Microbiology and Infectious diseases